Mai N. Tran1 and Russell R. Braeuer2
1Department of Biotechnology, School of Biotechnology, Vietnam National University Ho Chi Minh City International University, Ho Chi Minh City, Vietnam
22Department of Cancer Biology, the University of Texas M.D. Anderson Cancer Center, Houston, TX, USA 77054.
Editor: Huong Ha, Stanford University, Stanford, California, USA
* To whom correspondence should be addressed: Department of Biotechnology, School of Biotechnology, Vietnam National University Ho Chi Minh City International University, Ho Chi Minh City, Vietnam. Tel.: 848-3724-4270, Ext: 3233/3332; Email: tnamai@hcmiu.edu.vn
Abstract: While infectious diseases were a major concern in the world during the 20th century, cancer has become the most dangerous health problem of the 21st century. Treatment of infectious diseases and overall health has improved drastically over the past century, leading to prolonged life spans. However, with an aging world population, the incidence rates of cancer in developed and developing countries have increased. In general, cancer is the disease of uncontrolled generation of abnormal cells in the body. The genetically unstable nature of cancer cells allows them to become highly resistant to treatment. One of many tools to combat this problem is cancer patient surveillance. The United States of America and other developed countries are now collecting clinically relevant information about each and every patient. This data can be correlated with disease progression, treatment efficiency, environmental factors, or other variables. Scientific researchers in those countries have access to and analyze clinical samples for genetic mutations and gene expression profiling to identify other molecules of interest and compare it with disease stage and survival. The proper surveillance system of cancer patients is a powerful tool that must be used to understand the disease and improve cancer therapy and patient survival. Therefore, generating a successful surveillance system for cancer patients in developing countries such as Vietnam will have a profound effect on cancer control and potentially identify new ways to treat Vietnamese citizens.
Tóm tắt: Trong khi bệnh truyền nhiễm là mối lo ngại chính của thế giới trong thế kỉ 20 thì bệnh ung thư là vấn đề sức khoẻ nguy hiểm nhất của thế kỉ 21. Những phương pháp chữa trị bệnh truyền nhiễm và sức khoẻ tổng quát của con người đã được cải thiện rất nhiều trong thế kỉ vừa qua, tuổi thọ của con người vì thế cũng được nâng cao. Tuy nhiên, với dân số thế giới ngày càng già đi, tầng suất bệnh ung thư ở các nước phát triển và đang phát triển cũng tăng lên. Một cách tổng quát, bệnh ung thư là do sự sinh trưởng không kiểm soát được của những tế bào bất thường trong cơ thể. Sự bất ổn định của bộ gene của những tế bào ung thư giúp chúng có tính kháng cao với các liệu pháp chữa trị. Một trong những biện pháp để giải quyết vấn đề này là việc tầm soát bệnh nhân ung thư. Mỹ và các nước phát triển khác đang thu thập những thông tin lâm sàng của từng bệnh nhân càng nhiều càng tốt. Những thông tin này có thể được đối chiếu với tiến trình bệnh, hiệu quả của liệu pháp, các yếu tố môi trường và những yếu tố ảnh hưởng khác. Những nhà nghiên cứu khoa học ở các nước này có điều kiện để tiếp cận và phân tích những mẫu lâm sàng để tìm kiếm những đột biến gene và khảo sát biểu hiện gene để xác định những phân tử có tiềm năng và so sánh biểu hiện gene của những phân tử đó với cấp độ bệnh và tỉ lệ sống sót. Vì vậy một hệ thống tầm soát hợp lý cho bệnh nhân ung thư là một công cụ hữu dụng cần thiết để hiểu về bệnh và cải thiện liệu pháp chữa trị và tỉ lệ sống sót cho bệnh nhân. Do đó, việc thiết lập một hệ thống tầm soát cho bệnh nhân ung thư ở các nước đang phát triển như Việt Nam sẽ rất quan trọng và hữu ích đối với việc kiểm soát bệnh ung thư cũng như giúp phát triển những biện pháp chữa trị ung thư mới thích hợp cho người Việt.
Keywords: cancer, surveillance, research, Vietnam.
Các cụm từ viết tắt: DNA, deoxyribonucleic acid; GMCs, Genetically Modified Crops.
General information about cancer
Cancer is a disease of aberrant genetic alterations that triggers the uncontrolled proliferation of abnormal cells within organs of the body. As a result, the organs malfunction, generating serious health problems and/or become deleterious to the patients. More importantly, cancer cells from one organ can spread to other organs in the body through the blood and lymphatic systems, a process termed metastasis. In fact, the majority of cancer patients die due to metastases (1-5).
Cancer cells originate from normal cells in which the mutation of critical genes induces the accumulation of more mutations and the deregulation of several genes, thus generating genetic instability. Genetic instability and proliferation of cancer cells result in a tumor that consists of multiple cells with different genetic materials. Selection pressure from the microenvironment surrounding the tumor results in the formation of cancer cells that have the growth advantage and the ability to survive in any hostile microenvironment. Some tumors do not progress further than a mass of cells and are considered benign. Benign tumors only localize within the primary lesion, do not spread to other organs, and do not come back once removed. Malignant tumors, on the other hand, are cancerous. Malignant cancer cells invade nearby tissue and metastasize to distant organ sites (1-5).
Cancer can develop in any organ throughout the body and is named for the organ or the type of cells where it originated from (1, 3). In general, cancerous tumors are classified into two main types: solid tumors and liquid tumors. Solid tumors are tumors of solid tissues, consisting of two types: carcinomas and sarcomas. Carcinoma is the cancer of the epithelium lining inside and outside of the organ (5). Sarcoma is the cancer of connective tissues such as fat, bone, tendons and any type of tissues that connect, support and surround organs in the body (5, 6). Liquid tumors are tumors of the blood and lymphatic systems, consisting of leukemia, lymphoma and myeloma (5). Leukemia disperses as single cell population in the blood stream (7). Lymphomas start out as liquid tumors but usually aggregate to form solid tumor mass in the lymph nodes, spleen, bone marrow and other sites (8). Myelomas also form tumors in the bone marrow (9) (Figure 1).
There are multiple factors involved in cancer occurrence and development, including genetic background, and outside factors such as nutrition, personal habits, and the environment. Outside factors are classified into voluntary factors such as bad personal habits (cigarette smoking, and alcohol consumption), fatty diet, and sexual behavior and involuntary factors such as UV exposure, polluted air and contaminated drinking water (5).
There are five main therapies for cancer treatment: chemotherapy, radiotherapy, surgery, and targeted therapy. Chemotherapy and radiotherapy are the use of cytotoxic antineoplastic drugs or high-energy radiation, respectively; to eliminate cancer cells mainly by causing DNA damage, triggering a self-destruction program called apoptosis in cancer cells. These cytotoxic effects of chemo - and radiotherapy may also create mutations in normal cells that eventually can lead to cancer (10, 11). As a result, these therapies should be prescribed with consideration. Surgery is the oldest form of cancer treatment. Surgery is applied to remove the whole tumors, either cancerous or precancerous tumors, from patients to cure or prevent cancer. Patients can undergo surgery by itself or in combination with other cancer therapies. Targeted therapy is the newest form of treatment that is developed based on human knowledge about the molecular aspect of cancer biology. Targeted therapy is the use of small molecule inhibitors or antibodies to block the activity of critical protein molecules involved in the growth, spread and death avoiding machinery of cancer (12). The main advantage of targeted therapy is that they focus to the specific cellular and molecular changes of cancer cells; therefore, it may be more effective and less harmful to normal cells than chemotherapy and radiotherapy. However, drugs for targeted therapy are only available for some specific types of cancer and usually very expensive. Examining the expression of specific genes that are important for cancer progression in patient specimen biopsies can categorize patients and select the best therapeutic regimen. The most effective treatment however is early detection as this always brings greater chances of cancer cure. Maintaining frequent health examinations is a good way to prevent cancer.
The power of cancer surveillance and research in America
Before the proper amount of funding and research can be allocated for a given disease, the given society must first fully determine the detrimental effect of the disease on the population. Therefore, roper surveillance as well as the facilities needed for surveillance have to be established. According to the American cancer society website, cancer surveillance is defined as “the ongoing, timely, and systematic collection and analysis of information on new cancer cases, extent of disease, screening tests, treatment, survival, and cancer deaths” (13). These data are collected by many different systems and registries throughout America (13). Population-based registries collect the information from multiple reporting facilities within the given region of the United States (13). This can then be used to analyze the incidence rates, survival, and deaths. Also, cancer incidence rates among specific geographic regions, jobs, gender, ethnic groups, age, and its association with risk factors including infectious diseases such as HPV and Hepatitis B, tobacco smoking, and sun exposure are collected.
These data are then gathered across America and is published by agencies such as the National Center for Health Statistics (NCHS) by the Center for Disease Control and Prevention (CDC) and the Surveillance, Epidemiology, and End Results (SEER) Program of the National Cancer Institute (NCI) (Table 1). As publicly open data, it can then be analyzed, summarized, and published by professionals to discuss the overall incidence of cancer within the population (14), or this information can be used to focus on a specific event and its association with cancer. For example, thanks to cancer surveillance, we know that approximately 228, 190 new lung cancer cases and another 118,080 deaths will occur during 2013 (14). Data collection of smokers vs. non-smokers suggests that 85% of lung cancers are associated with smoking (15). With this information, we now know that lung cancer is one of the most prevalent cancers in America and we can propose that if Americans stop smoking lung cancer prevalence will be drastically reduced and overall health will improve.
Although the association of lung cancer with smoking is a perfect example for attacking cancer prevention by simply knowing the population’s life habits, genome and molecular analysis over the past decade have taken cancer surveillance to the next level. For example, women in America who are born with the mutation of a specific gene called BRCA1 have a much higher chance of developing breast cancer (16). Therefore, women who possess this mutation should be watched much more closely and screened more often than women with the normal BRCA1 gene. Other variables, such as race and ethnicity, are also considered to determine whether a specific race is more likely to have the BRCA1 mutation. One study of Hispanic women in the southwest region of the United States who have personal or familial history of breast cancer had a 25% prevalence of the BRCA1 gene deletion, therefore, BRCA1 mutations in Hispanic women should be screened as vigorously as in other ethnicities (17). Analysis of cancer cell specific genetic mutations that are not found in normal cells has also become an important tool for cancer treatment by revealing new potential molecular targets for targeted therapy. At the turn of the century, by studying the protein coding portion of genes in numerous melanoma cell cultures and primary tumors collected from patients, it was discovered that the gene BRAF is mutated in approximately 60% of melanoma (skin cancer) patients (18). The mutated gene leads to an activated BRAF protein that enhances melanoma growth and metastasis. Targeting specifically the mutant BRAF protein and not the wild type BRAF protein in normal cells with small molecular inhibitors such as vemurafenib has proved advantageous. However, current data shows that melanoma patients relapse after 6-7 months of treatment (19). Nonetheless, this is a step in the right direction, and the addition of other small molecular inhibitors targeting other genes could improve survival.
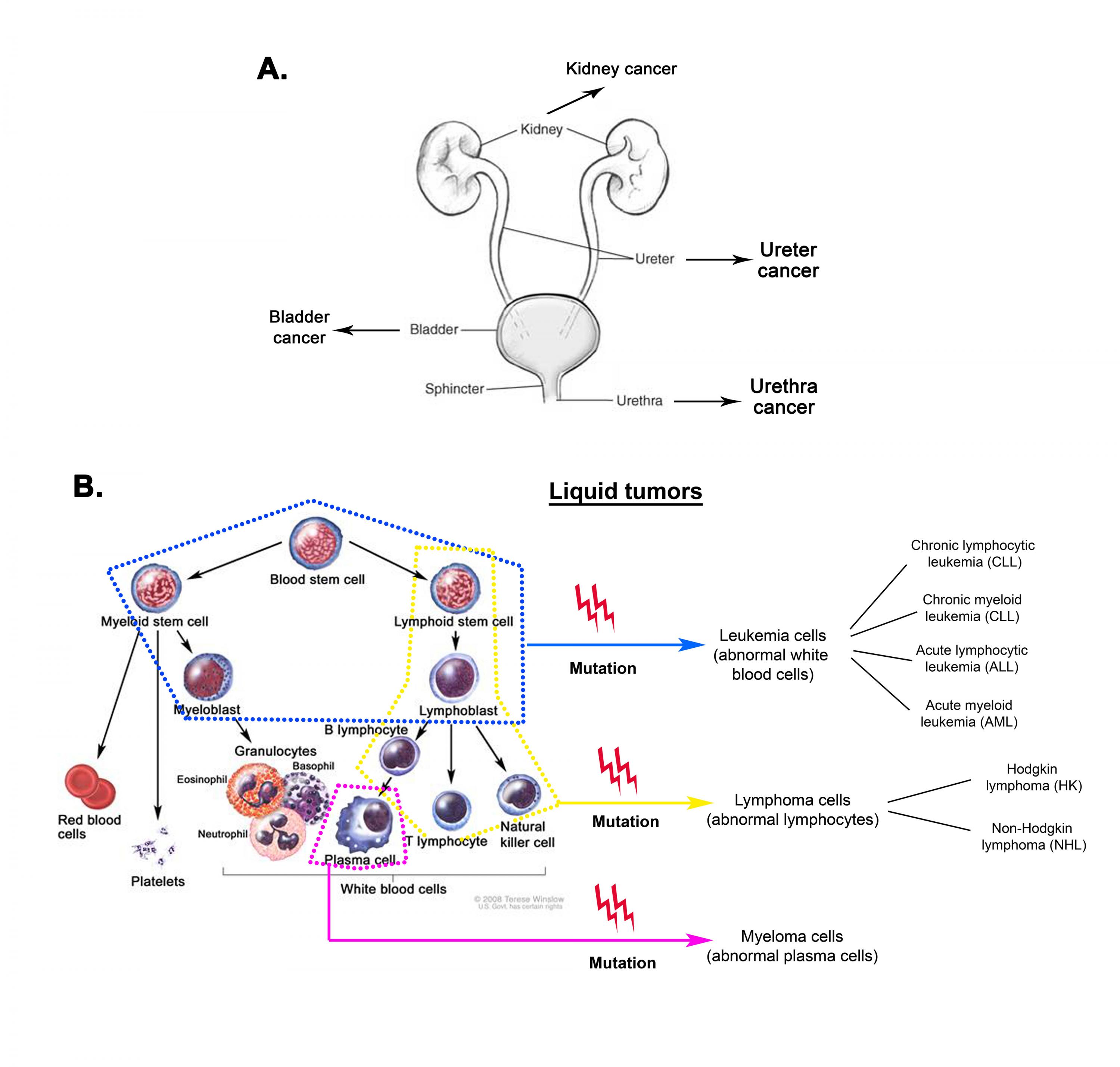
Figure 1: Solid and liquid tumors. A. Carcinoma of the urinary system. Cancer can occur anywhere along the urothelium, an epithelial layer lining the urinary tract. Cancer of the urothelium is referred to as urothelial carcinoma. (Adapted from National Kidney and Urologic Diseases Information website). B. Types of liquid tumors and their origins. Mutations of different cells in the hematopoietic system generate different types of leukemia, lymphoma and myeloma. (© 2008 Terese Winslow, U.S. Govt. has certain rights).
Through the cooperation and collaboration of several research scientists, doctors, departments, hospitals, registries, cities, and states cancer surveillance has become a reliable and absolutely necessary tool in combating the disease. The discoveries mentioned above could not have been accomplished without surveillance, and future discoveries will rely on these data. Currently the cancer genome atlas (TCGA) project is collecting large amounts of patient data on many different cancers. This information will be another powerful tool and will be available for all scientists and medical hospitals to further identify new targets for cancer therapy.
Cancer status in Vietnam
While the 20th century is the century of infectious diseases, the 21st is the century of cancer, heart diseases and other non-infectious diseases. This is the fact not only in developed countries but also in developing countries including Vietnam, albeit specific diseases still require a tremendous amount of attention. In Vietnam, even though cancer has been considered as a major health problem since the 1990s (20), it only became a social concern in the 2000s. There are two main sources for cancer statistics, the Hanoi Cancer Registry, established in 1987, is the data source for the North of Vietnam, and the Ho Chi Minh City Cancer Registry, established in 1990, is the data source for the South of Vietnam. The Cantho Cancer Registry, established in 2001, is another data source for the South. The age standardized rate (ASR) of all site cancer incidence in males and females in three periods of time, 1993-1998, 2001-2004, and 2006-2007, demonstrates an increasing trend in cancer incidence in the whole country, from 151.1/105 (1993-1998) to 160.0/105 (2006-2007) for males and from 106.8/105 to 143.9/105 for females (21). This increasing trend can be explained by multiple reasons including polluted environment, tobacco smoking, spreading of infectious diseases, as well as advances in cancer diagnosis and social awareness of the disease. During the three time periods, lung is always the most common cancer site in males, followed by stomach and liver (21). In females, cancer of the cervix was the most common in 1993-1998; however, breast cancer is now the most common type, followed by cervical and lung cancer (Table 2) (21). The high incidence of lung cancer in both males and females is mainly due to the high consumption of tobacco in Vietnam. In 1995, 73.4% of male and 3.9% of female Vietnamese are smokers (22). This “smoking culture” leads to multiple diseases for the respiratory system including cancer. Liver cancer is ranked 3rd in males and 8th in females for cancer incidence. Hepatitis B virus (HBV) infection is a strong risk factor for liver cancer and a high prevalence of HBV infection has been reported in 8.8 to 19.0% of adult Vietnamese (23, 24). Similar to other developing countries, Vietnam still has poor social awareness of nutritional hygiene as well as sexual transmitted diseases (STDs) such as HPV infection. This is one of the explanations for high stomach and cervical cancer incidence in Vietnam.
| Males | Incidence1 | Females | Incidence1 |
|---|---|---|---|
| Prostate | 152 | Breast | 123.8 |
| Lung and Bronchus | 74.3 | Lung and Bronchus | 51.9 |
| Urinary Bladder | 36.6 | Colorectal | 291 |
| Colorectal | 36.1 | Uterine Corpus | 23.6 |
| Melanoma of the Skin | 27.4 | Thyroid | 18.2 |
1 The incidence is per 100,000 men or women and are age-adjusted to the 2000 US standard population.
Table 1. Top 5 Most Prevalent Cancers in the United States (2006-2010). The 5 most prevalent cancers in men and women within the United States are shown. Prostate and Breast cancer have the highest incidence. The prostate and uterine corpus (endometrial cancer) are gender specific. Although men can have breast cancer, the vast majority of breast cancer patients are women. Colorectal and Lung cancer are highly prevalent in both genders. Data is according to the SEER Cancer Statistics Review (1975-2013).
| Males | 2006-2007 Incidence1 | Females | 2004-2006 Incidence1 |
|---|---|---|---|
| Lung and Bronchus | 27.3 | Breast | 32.80 |
| Stomach | 23.0 | Cervix Uteri | 16.25 |
| Liver | 21.98 | Lung and Bronchus | 10.5 |
| Colorectal | 10.15 | Stomach | 10.1 |
| Pharynx | 8.74 | Colorectal | 8.5 |
1 The incidence is per 100,000 men or women. Data was collected and published by Vuong et al. 2010 and was age-adjusted on the basis of the world standard population.
Table 2. Top 5 Most Prevalent Cancers in Vietnam. The 5 most prevalent cancers in men and women within Vietnam are shown. The most prevalent cancer in women is Breast cancer. Cancers of the liver and gastrointestinal tract are highly prevalent (liver cancer is the 6th most prevalent cancer in women).
The rise in cancer incidence has not gone unnoticed in Vietnam. The Vietnamese government has been fostering cancer prevention and treatment programs in Vietnam since the 1990s with the tobacco control program in 1989, HBV vaccination in the extended program of immunization for newborns in Hanoi and Ho Chi Minh City since 1997, public education on nutrition and nutrition hygiene as well as safe sex and sexual transmitted diseases, introduction of the PAP test for cervical cancer and STDs prevention, and a breast cancer screening program in the late 1990s to early 2000s (25). Currently, Vietnam has five cancer specific hospitals and cancer specialized departments in more than 20 general hospitals throughout the country. However, these facilities poorly fulfill the high demand of cancer care in Vietnam due to the limited and outdated instruments and the lack of trained oncologists. The economic difficulties hinder cancer research that requires large amounts of funding and a long-term investment. Despite the effort of cancer education from the government to the Vietnamese citizens, social awareness of the disease is still very poor.
Conclusion
Cancer and its intrinsic complicated biology is inevitably a great challenge for disease control and prevention. Although there are cancer registries in Ho Chi Minh City and Hanoi, there is still a need for a more systematic registry that encompasses not only two of the largest cities in Vietnam, but also the surrounding communities and towns. An improved and consistent surveillance system in all participating clinics and hospitals would be advantageous. Therefore, data from different registries could be more easily combined for the surveillance of cancer in all of Vietnam. These registries should include prevalence of cancer in different genders, age, location, and their correlation with risk factors. A more progressive approach would also be to identify significant genetic alterations in these cancers, compare them with the data of developed countries, and determine if current known treatment modalities are available for Vietnamese cancer patients. If not, exome analysis (analysis of the protein coding genes), gene copy, and gene expression analysis would be a good start to discover new genes that are critical for the development of cancer in Vietnamese individuals. With a better understanding of the incidence of cancer within the population, it’s correlation with viral infections, smoking, or genetic aberrations, scientists and health professionals can lead the way with new discoveries and improved clinical advice to prevent and treat cancer patients in Vietnam.
References:
- Simon H-U, Haj-Yehia A, &anp; Levi-Schaffer F (2000) Role of reactive oxygen species (ROS) in apoptosis induction. Apoptosis 5(5):415-418.
- Anonymous (Metastatic Cancer. (National Cancer Institute).
- Anonymous (2006) What you need to know about cancer (National Institutes of Health), (Institute NC).
- Hanahan D & Weinberg RA (2011) Hallmarks of cancer: the next generation. (Translated from eng) Cell 144(5):646-674 (in eng).
- Weinberg RA (2007) The biology of cancer (Garland Science, Taylor & Francis Group, LLC).
- World Bank (
- Anonymous (2008) What you need to know about Leukemia (National Institutes of Health), (Institute NC).
- Anonymous (2008) What you need to know about Non-Hodgkin Lymphoma (National Institutes of Health), (Institute Nc).
- Anonymous (2008) What you need to know about Multiple Myeloma (National Institutes of Health), (Institute NC).
- Rudan I, Boschi-Pinto C, Biloglav Z, Mulholland K, & Campbell H (2008) Epidemiology and etiology of childhood pneumonia. (Translated from eng) Bull World Health Organ 86(5): 408-416 (in eng).
- Anonymous (2007) Chemotherapy and You: Support for People With Cancer. (National Cancer Institute).
- Anonymous (2012) Targeted Cancer Therapies. (National Cancer Institute).
- Anonymous (2012) Cancer Surveillance Programs in the United States. (American Cancer Society).
- Siegel R, Naishadham D, & Jemal A (2013) Cancer statistics, 2013. CA: a cancer journal for clinicians 63(1): 11-30.
- Warren GW & Cummings KM (2013) Tobacco and lung cancer. American Society of Clinical Oncology educational book / ASCO. American Society of Clinical Oncology. Meeting 2013: 359-364.
- Easton DF, Ford D, & Bishop DT (1995) Breast and ovarian cancer incidence in BRCA1-mutation carriers. Breast Cancer Linkage Consortium. American journal of human genetics 56(1): 265-271.
- Weitzel JN, et al. (2013) Prevalence and type of BRCA mutations in Hispanics undergoing genetic cancer risk assessment in the southwestern United States: a report from the Clinical Cancer Genetics Community Research Network. Journal of clinical oncology: official journal of the American Society of Clinical Oncology 31(2): 210-216.
- Davies H, et al. (2002) Mutations of the BRAF gene in human cancer. Nature 417(6892): 949-954.
- Sosman JA, et al. (2012) Survival in BRAF V600-mutant advanced melanoma treated with vemurafenib. The New England journal of medicine 366(8): 707-714.
- Ngoan le T (2006) Cancer mortality in a Hanoi population, Viet Nam, 1996-2005. Asian Pacific journal of cancer prevention: APJCP 7(1): 127-130.
- Vuong DA, Velasco-Garrido M, Lai TD, & Busse R (2010) Temporal trends of cancer incidence in Vietnam, 1993-2007. Asian Pacific journal of cancer prevention: APJCP 11(3):739-745.
- Dai Xuan Pham NHD, Hoang Trong Truong, Jenkins C. (1995) A tobacco use prevalence survey. Vietnam: a tobacco epidemic in the making, Hanoi), pp 45-66.
- Duong TH, Nguyen PH, Henley K, & Peters M (2009) Risk factors for hepatitis B infection in rural Vietnam. Asian Pacific journal of cancer prevention: APJCP 10(1):97-102.
- Nguyen VT, McLaws ML, & Dore GJ (2007) Highly endemic hepatitis B infection in rural Vietnam. Journal of gastroenterology and hepatology 22(12): 2093-2100.
- Anh PT & Duc NB (2002) The situation with cancer control in Vietnam. Japanese journal of clinical oncology 32 Suppl: S92-97.
About the author: Dr. Mai Tran received her PhD in Cancer Biology/Health Sciences from the University of Texas – MD Anderson Cancer Center in 2013. She is interested in transcriptional control, markers for cancer progression and metastasis, and the biology of bladder cancer. Her PhD thesis is about the role of p63, a transcription factor, in bladder cancer. After finishing her PhD, Dr. Mai Tran returned to Vietnam, her home country, and is now a faculty of the Department of Biotechnology, School of Biotechnology, Vietnam National University Ho Chi Minh City International University.

Comments
Anh Pham replied on Permalink
Cancer statistic from Vietnam
Mai Tran replied on Permalink
Cancer statistic in Vietnam
Add new comment